Understanding Fatty Liver Disease
Clear, Evidence-based information on causes, diagnosis, and treatment.

Fatty liver disease occurs when excess fat builds up inside liver cells. It often develops silently and is closely linked to metabolic health, including conditions such as obesity.
Overview
What is the liver's function?
Your liver is an essential organ responsible for over 500 vital functions. A healthy, functioning liver is critical for human health. The most significant functions include:
- Producing bile, which aids digestion
- Producing proteins essential for the body
- Storing vitamins and minerals
- Converting nutrients into energy
- Metabolism of proteins, carbohydrates, and fats
- Storing and releasing glucose as needed
- Regulates blood clotting
- Detoxifying and breaking down toxins, including alcohol and waste products
What are the different forms of fatty liver disease?
There are two main categories of fatty liver disease, based on the underlying cause:
-
Alcohol-associated liver disease (ALD):
Fatty liver disease caused by regular or excessive alcohol consumption. Alcohol can lead to fat accumulation in the liver and, over time, inflammation, fibrosis, cirrhosis, or liver failure. -
Metabolic dysfunction–associated steatotic liver disease (MASLD):
Formerly known as nonalcoholic fatty liver disease (NAFLD), MASLD is not caused by alcohol use. Instead, it is associated with metabolic conditions such as obesity, insulin resistance, type 2 diabetes, high blood pressure, and abnormal cholesterol levels. MASLD affects approximately one in three adults and an increasing number of children in the United States.When MASLD progresses to liver inflammation and injury, it is referred to as metabolic dysfunction–associated steatohepatitis (MASH) (formerly NASH), which carries a higher risk of fibrosis, cirrhosis, and liver-related complications.
Stages of fatty liver disease
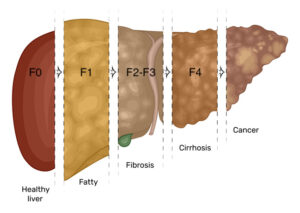
Not everyone with fatty liver disease will progress to advanced stages. Early identification and lifestyle changes can alter the course of the disease.
Causes, Signs, and Symptoms
What are the risk factors for developing fatty liver disease?
While some people develop fatty liver disease without obvious risk factors, most cases—particularly metabolic dysfunction–associated steatotic liver disease (MASLD)—are associated with one or more of the following:
-
Being overweight or obese
-
Type 2 diabetes or insulin resistance
-
Metabolic syndrome, including:
-
Insulin resistance
-
High blood pressure
-
Abnormal cholesterol levels
-
Elevated triglycerides
-
-
Genetic predisposition
-
Polycystic ovary syndrome (PCOS)
-
Growth hormone deficiency
-
A family history of fatty liver disease, obesity, or type 2 diabetes
Signs and Symptoms
Fatty liver disease often has no signs or symptoms, especially in the early stages. When symptoms do occur, they may include:
-
Generalized malaise or feeling unwell
-
Fatigue
-
Intermittent discomfort or pain in the upper right abdomen
As fatty liver disease progresses to advanced fibrosis or cirrhosis, additional signs and symptoms may develop, including:
-
Itchy skin
-
Abdominal swelling due to fluid buildup (ascites)
-
Mental confusion (hepatic encephalopathy) or extreme fatigue
-
Shortness of breath
-
Yellowing of the skin and eyes (jaundice)
-
Enlarged spleen
-
Swelling of the legs and/or genital area
-
Spider-like blood vessels on the skin (spider angiomas)
-
Nausea and loss of appetite
-
Unintentional weight loss
Diagnosis and Tests
How is fatty liver disease diagnosed?
Because fatty liver disease often causes few or no symptoms, it is frequently discovered incidentally during testing done for other reasons.
For example, routine blood work may show elevated liver enzymes, prompting further evaluation. In other cases, fatty liver disease is identified on imaging studies—such as an abdominal ultrasound ordered to evaluate gallbladder disease, or a CT scan performed for abdominal pain. Although the liver may not be the original reason for testing, fatty liver disease is often detected during this process.
Diagnosis and staging of fatty liver disease typically involve a combination of imaging and blood tests. These tests help confirm the presence of fat in the liver and assess disease severity. The specific tests ordered may vary based on provider preference, test availability, evolving clinical guidelines, and individual patient factors.
While liver biopsy remains the gold standard for diagnosing and staging fatty liver disease, it is not routinely required. Because biopsy is invasive, costly, and carries potential risks, it is generally reserved for patients at higher risk for advanced disease or when another underlying liver condition cannot be excluded using noninvasive testing.
Imaging
Imaging studies are commonly used to detect fatty liver disease and assess the degree of liver damage.
-
Abdominal Ultrasound – A noninvasive test used to evaluate the organs and structures within the abdomen. It is often the first imaging study used to detect fatty changes in the liver.
-
Computed Tomography (CT Scan) – Uses a combination of X-rays and computer technology to create detailed cross-sectional images of the liver and surrounding structures. CT scans can identify fatty infiltration and evaluate for other liver abnormalities. Contrast is sometimes used to enhance image detail.
-
Magnetic Resonance Imaging (MRI) – Produces highly detailed images of the liver using a powerful magnet and radio waves. MRI is more sensitive than ultrasound or CT for detecting liver fat.
-
Magnetic Resonance Elastography (MRE) – An advanced MRI-based technique that combines imaging with low-frequency vibrations to create a visual map (elastogram) of liver stiffness. MRE is one of the most accurate noninvasive tools for assessing liver fibrosis and inflammation.
-
FibroScan® (Transient Elastography) – A specialized ultrasound-based test that measures liver stiffness and fat content. It is commonly used to stage fibrosis and monitor disease progression or improvement over time.
Blood Tests
Blood tests help evaluate liver function, metabolic health, and possible causes of liver injury. No single blood test can diagnose MASLD or MASH on its own, but together they provide important clues.
Common Blood Tests
-
Complete Blood Count (CBC)
Looks at red blood cells, white blood cells, and platelets. Low platelets can be a sign of advanced liver disease. -
Hemoglobin A1c (A1c)
Measures average blood sugar over 3 months. Higher levels are commonly associated with MASLD and MASH. -
Lipid Panel
Measures cholesterol and triglycerides, which are often elevated in metabolic liver disease. -
Comprehensive Metabolic Panel (CMP)
Includes electrolytes, kidney function, and liver-related values such as bilirubin and albumin. -
Prothrombin Time / INR (PT/INR)
Assesses blood clotting, which can be affected when liver function declines.
Liver Enzymes
Liver enzymes are released into the blood when liver cells are stressed or injured.
-
ALT (Alanine Aminotransferase)
Most specific to the liver and often elevated early in liver disease. -
AST (Aspartate Aminotransferase)
Found in the liver and other tissues; elevations may indicate liver injury. -
Alkaline Phosphatase (ALP)
Can rise with bile duct problems or certain liver conditions. -
GGT (Gamma-Glutamyl Transferase)
Often elevated with liver disease and alcohol exposure; helps clarify the source of abnormal ALP. -
Bilirubin
A yellow pigment processed by the liver. Elevated levels can cause jaundice and signal impaired liver function.
Additional Testing (When Needed)
If liver enzymes are persistently elevated, additional blood tests may be ordered to rule out other treatable liver conditions, such as:
-
Viral hepatitis (A, B, C)
-
Autoimmune liver disease
-
Alpha-1 antitrypsin deficiency
-
Wilson’s disease
-
Hemochromatosis (iron overload)
Calculated Liver Scores
Some blood tests are combined into scores that help estimate liver severity:
-
FIB-4 Score
A noninvasive estimate of liver fibrosis based on age, AST, ALT, and platelet count.-
Low score → minimal fibrosis
-
Higher score → increased risk of advanced fibrosis
-
-
MELD 3.0 Score
Used only in advanced liver disease to assess severity and transplant priority.
Liver Biopsy
A liver biopsy is a procedure in which a small sample of liver tissue is removed and examined under a microscope. This allows for detailed evaluation of inflammation, scarring (fibrosis), and other underlying liver conditions.
While a liver biopsy is considered the gold standard for diagnosing and staging liver disease, it is not routinely required for most people with MASLD or MASH. It is typically reserved for select cases when the diagnosis is unclear or when results will significantly impact treatment decisions.
Sedation is usually provided to improve comfort during the procedure.
Common Types of Liver Biopsy
-
Percutaneous (most common)
A thin needle is inserted through the abdominal wall to obtain a small sample of liver tissue. -
Transjugular
A vein in the neck is used to access the liver and obtain a tissue sample. This method is often chosen for people with ascites, bleeding or clotting disorders, or advanced liver disease. -
Laparoscopic
Performed during abdominal surgery (such as gallbladder removal), allowing a liver biopsy to be completed at the same time.
Management and Treatment
How is fatty liver disease treated?
Management of fatty liver disease focuses on treating the underlying metabolic conditions that contribute to liver fat accumulation and inflammation, including obesity, insulin resistance, type 2 diabetes, and metabolic syndrome. Dietary changes, physical activity, and sustainable lifestyle modification remain the foundation of treatment for metabolic dysfunction–associated steatotic liver disease (MASLD) and metabolic dysfunction–associated steatohepatitis (MASH). Bariatric surgery may be an option for select individuals.
In March 2024, the FDA granted accelerated approval to resmetirom (Rezdiffra) as the first medication approved for the treatment of adults with MASH and moderate to advanced liver fibrosis (stages F2–F3). This medication is used in combination with dietary and lifestyle modification and represents an important advancement in the medical management of MASH.
Additional medications—including therapies originally approved for diabetes and obesity—have demonstrated benefits for liver health and are increasingly used as part of a comprehensive treatment approach. These options are discussed in more detail below.
Dietary Recommendations
The Standard American Diet is a major contributor to the development and progression of fatty liver disease. Diets high in ultra-processed foods, added sugars, and refined carbohydrates promote insulin resistance, inflammation, and fat accumulation in the liver—contributing not only to the development of fatty liver disease, but also to progression to more advanced stages. (And yes, the irony of the acronym “SAD” is not lost on me.)
The Mediterranean diet has long been recommended as an effective dietary approach for slowing progression and, in some cases, improving fatty liver disease. This eating pattern emphasizes whole, nutrient-dense foods such as vegetables, fruits, legumes, nuts, olive oil, fatty fish, white meat, and minimally processed whole grains, while limiting ultra-processed foods, sweets, processed meats, and red meat.
The Mediterranean diet is rich in antioxidants and anti-inflammatory compounds, which support liver health and improve insulin sensitivity. Beyond liver benefits, this dietary pattern has been associated with reduced risk of cardiovascular disease, type 2 diabetes, cognitive decline, and chronic inflammation, while supporting better sleep, cognition, and overall longevity.
Importantly, the Mediterranean diet is not overly restrictive and allows for cultural and regional variation, making it a sustainable long-term lifestyle rather than a short-term diet.
Coffee
Coffee is one of the most widely consumed beverages in the world, and fortunately, there is strong evidence that it is beneficial for liver health. Research shows that people who drink coffee have a lower risk of developing fatty liver disease in the first place. Among those who already have fatty liver disease, coffee appears to have a protective effect by reducing liver inflammation and slowing the progression of fibrosis—the scarring process that can ultimately lead to cirrhosis.
Even among individuals with established cirrhosis, coffee consumption has been associated with lower liver-related mortality. In short, when it comes to liver health, coffee keeps getting better.
Is decaf good for your liver?
Unfortunately, most of the liver-protective benefits appear to be linked to caffeine. During caffeine metabolism, the body produces a compound called paraxanthine, which has been shown to slow the development of liver fibrosis. In addition to caffeine, coffee contains more than 1,000 biologically active compounds, and research is ongoing to determine which of these contribute to its liver benefits.
How much coffee is recommended?
Most studies suggest that at least 2 cups per day are needed to see liver-protective effects. In one study, consuming 2 cups daily was associated with a 44% reduction in the risk of cirrhosis, while 4 cups daily reduced the risk by up to 65%.
That said, not everyone tolerates this amount of coffee. Individuals with heart rhythm issues, significant anxiety, insomnia, or other caffeine sensitivity should avoid forcing higher intake and should discuss coffee consumption with their healthcare provider.
To maximize benefit, skip the creamers, sugar, and artificial sweeteners. Stick with black coffee when possible—organic if available.
Intermittent Fasting/Time Restricted Eating
Time-restricted eating (TRE) and intermittent fasting (IF) are increasingly recognized as effective tools for improving metabolic health and reducing liver fat in people with fatty liver disease. These approaches focus on when food is consumed rather than strictly what is eaten, and have been shown to improve insulin sensitivity, promote weight loss, and reduce liver inflammation—key drivers of MASLD and MASH.
Intermittent fasting involves alternating periods of eating with planned periods of fasting, most commonly through a daily eating window (for example, eating within an 8–10 hour window and fasting the remaining hours). This structured reduction in eating time allows the liver to shift away from constant glucose and insulin exposure, supporting metabolic repair and fat mobilization.
Fasting has been practiced for centuries for cultural and religious reasons, but modern research now supports its role in metabolic disease management. Emerging evidence suggests that when you eat can be just as important as what you eat, particularly for liver health.
Important safety note:
Intermittent fasting may be beneficial for individuals with fatty liver disease without advanced liver disease, but it is not recommended for patients with cirrhosis, who require more consistent caloric and protein intake to prevent muscle loss and complications. As with any dietary strategy, fasting should be individualized and discussed with a healthcare provider.
Exercise
Exercise provides meaningful benefits for liver health independent of weight loss. Research shows that physical activity can reduce liver fat, improve insulin sensitivity, and lower inflammation—even when the number on the scale doesn’t change.
While studies vary on the optimal type and intensity of exercise, consistent moderate-intensity activity totaling at least 150 minutes per week, ideally spread over 4–5 sessions, has been shown to improve or prevent fatty liver disease. Examples include walking, hiking, swimming, cycling, mowing the lawn, or gardening.
Some evidence suggests that higher-intensity exercise may offer additional benefit, particularly for reducing liver fibrosis. Activities such as running, brisk walking, HIIT (high-intensity interval training), stair climbing, resistance training, burpees, or cross-country skiing fall into this category. That said, intensity should always be tailored to an individual’s fitness level and medical conditions.
The greatest and most sustainable improvements in liver health occur when exercise is combined with dietary and lifestyle changes.
And remember—you can’t outrun a bad diet.
Bariatric Surgery
Weight Loss Surgery: Benefits and Limitations
Bariatric surgery includes invasive procedures used to treat obesity and obesity-related conditions. Fatty liver disease is increasingly recognized as an obesity-related condition that may benefit from surgical weight loss.
Accepted criteria for bariatric surgery include a BMI ≥ 40 kg/m² without additional medical conditions, or a BMI ≥ 35 kg/m² in the presence of comorbidities such as type 2 diabetes, uncontrolled hypertension, osteoarthritis, or urinary incontinence. Growing evidence suggests that bariatric surgery can significantly improve hepatic steatosis and may improve liver inflammation and fibrosis in appropriately selected patients.
The most common bariatric procedures include sleeve gastrectomy and Roux-en-Y gastric bypass. Less invasive, endoscopic bariatric therapies are an emerging area of interest and may expand treatment options in the future. Individuals with cirrhosis are at increased risk for postoperative complications and mortality, and careful preoperative evaluation is essential.
Bariatric surgery is a tool, not a cure. While many individuals experience durable weight loss and metabolic improvement, long-term success depends heavily on sustained lifestyle changes. Habits are difficult to break — and unfortunately, behavior modification isn’t included in the surgical package 😉.
Alcohol
How much is too much?
Complete alcohol cessation is generally recommended for individuals diagnosed with fatty liver disease. Even low levels of alcohol intake have been associated with increased liver fibrosis and reduced likelihood of disease improvement—particularly in patients with obesity or metabolic risk factors.
Alcohol intake is often categorized as follows:
-
Mild: up to 20 g/day for women, up to 30 g/day for men
-
Moderate: 21–39 g/day for women, 31–49 g/day for men
-
Heavy: ≥40 g/day for women, ≥50 g/day for men
Importantly, what is commonly considered “mild” alcohol intake is not benign in the setting of fatty liver disease. Studies show that even mild intake is associated with increased fibrosis and less reversal of liver fat.
Alcohol’s impact varies widely between individuals and depends on multiple factors, including type of alcohol, total amount, drinking pattern, frequency, and duration of use.
A study published in January 2024 found that patients with early-stage fatty liver disease could consume less than 7.4 grams of alcohol per day without increasing their risk of progression to advanced liver disease. Notably, 7.4 grams is less than half of what is traditionally defined as “mild” alcohol intake.
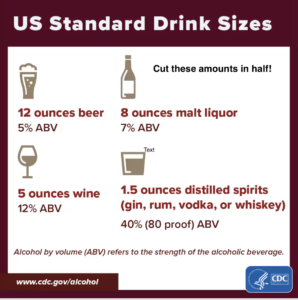
So what does 7.4 grams of alcohol actually look like?
-
~6 ounces of beer
-
~2.5 ounces of wine
-
<1 ounce of distilled spirits (vodka or tequila)
To put this into perspective, review the image below and cut the standard serving sizes in half. The amounts are surprisingly small—making it very easy to unintentionally exceed a “safe” threshold.
For most people with fatty liver disease, avoiding alcohol altogether is the safest and most effective choice, with rare exceptions. The long-term effects of low-level alcohol use in fatty liver disease continue to be studied.
Medications
Current Medications
In March 2024, the FDA granted accelerated approval to resmetirom (Rezdiffra) as the first treatment for adults with MASH and moderate-to-advanced liver fibrosis (F2-F3), to be used in combination with diet and lifestyle modification. In August 2025, semaglutide (Wegovy) received FDA approval for the treatment of adults with MASH and F2-F3 fibrosis without cirrhosis, becoming the first GLP-1 receptor agonist approved for this indication.
These medications work through different mechanisms and may be appropriate for different patients depending on fibrosis stage, metabolic profile, and comorbid conditions.
The chart below includes medications approved for treatment of other medical conditions that have shown some benefits for treatment of fatty liver disease.
FDA-approved treatments for MASH
| Medication | Indication |
|---|---|
| Resmetirom (Rezdiffra) | MASH with F2–F3 fibrosis |
| Semaglutide (Wegovy) | MASH with F2–F3 fibrosis (without cirrhosis) |
Medications approved for other conditions with potential liver benefit
| Medication | Primary Indication |
|---|---|
| Vitamin E | Selected patients (non-diabetic, non-cirrhotic) |
| Pioglitazone | Type 2 diabetes |
| Liraglutide | Diabetes / Obesity |
| Tirzepatide | Diabetes / Obesity |
| SGLT-2 inhibitors | Type 2 diabetes |
The medications listed above are approved for the treatment of metabolic conditions that commonly coexist with fatty liver disease. Several have demonstrated improvements in liver fat, inflammation, and metabolic risk factors, but are not currently FDA-approved specifically for MASH unless otherwise noted.
Future Medications
There are multiple medications currently in various stages of clinical trials targeting inflammation, fibrosis, and metabolic dysfunction in MASH. This remains a rapidly evolving area of research, and additional treatment options are expected in the coming years.